
Elbow Dislocation
Elbow Dislocation
Morganne Murphy-Meyers, MS4; Brian Gilmer, MD
Case Example:
A 17-year-old male presents with right elbow pain and a visible elbow deformity following a fall on an outstretched arm while playing football about 30 minutes ago. He is unable to move his arm due to pain. On physical exam, his right elbow is flexed with prominence of his olecranon and diffuse swelling around the joint. There are no injuries to the skin and the proximal and distal joints are normal appearing. He was neurovascularly intact distal to the elbow.
Introduction:
Elbow dislocation occurs when the humerus comes out of alignment with the bones of the forearm, the ulna and radius. Elbow dislocations are the second most common joint dislocation, other than shoulder dislocations, and are the most common joint dislocations in children1.
Anatomy:
The elbow is a complex synovial hinge joint consisting of an articulation between the distal humerus and proximal ulna (humeroulnar joint), distal humerus and proximal radius (humeroradial joint), and the ulna and radius (radioulnar joint)3. The humeroulnar joint is responsible for flexion and extension of the elbow3. The humeroradial joint and the radioulnar joint are responsible for pronation and supination of the forearm3.
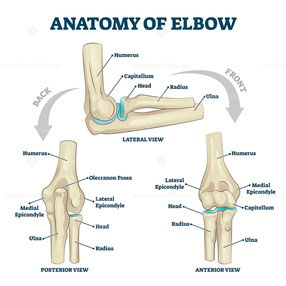
Normal anatomy of the elbow bones4.
The three main ligaments of the elbow consist of the radial collateral ligament connecting the lateral epicondyle of the humerus to the radial notch of the ulna, the ulnar collateral ligament connecting the medical epicondyle to the coronoid process and olecranon of the ulna, and the annular ligament of the radius surrounding the head of the radius and anchoring to the ulna.
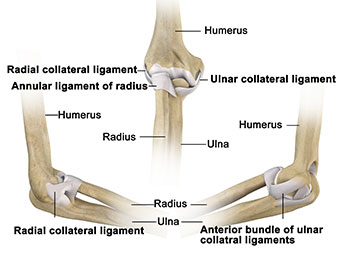
Normal anatomy of the elbow ligaments5.
There are three large nerves that travel over the elbow joint and are at risk of injury with elbow dislocation. They include the radial nerve, the median nerve, and the ulnar responsible for sensation and movements of the forearm and hand.
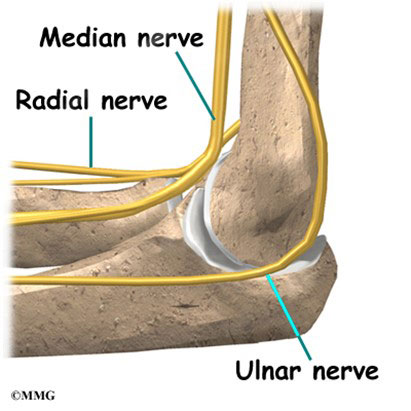
Normal anatomy of the elbow nerves6.
There are several blood vessels that anastomose over the elbow joint including the brachial artery, radial artery, ulnar artery, and deep brachial artery.
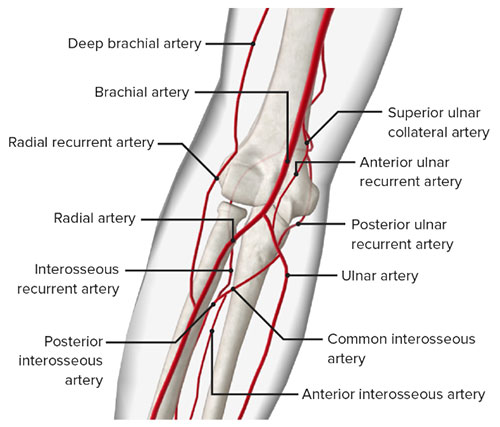
Normal anatomy of the elbow blood vessels7.
History:
Elbow dislocations are classified as non-complex if there is no associated fracture and complex if there is a fracture of one of the bones in the joint1. The most common elbow dislocation is posterolateral and is usually caused by a combination of axial loading, external rotation of the forearm, and a valgus posterolateral force1. Anterior elbow dislocations are rare but usually occur following a fall on a flexed elbow and a strong anterior force on the proximal ulna2.
Physical Exam:
On physical exam, the patient will have pain and swelling over the elbow joint. They will have an inability to extend and flex the joint. The normal three-point orientation of the olecranon, medial epicondyle, and lateral epicondyle when the elbow is flexed at 90 degrees.

Posterior Elbow Dislocation Physical Exam Findings8
A neurovascular exam should be completed on every patient with an elbow dislocation. The three nerves most commonly damaged (the ulnar, radial, and median) should be evaluated with the following maneuvers:
- Sensation over the nerve regions:
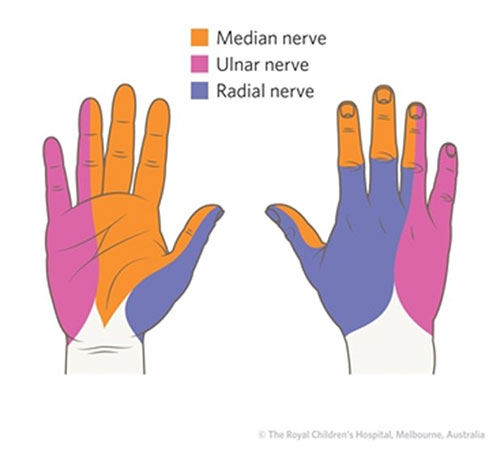
Sensory innervation of the hand9.
- Motor function:
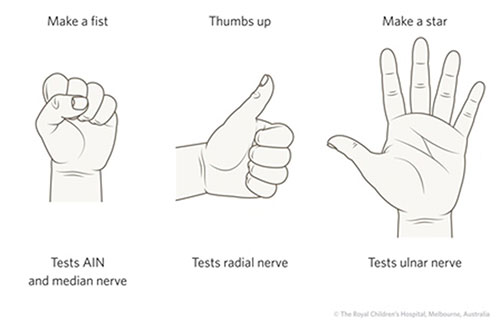
Motor exam maneuvers of the hand9
Injury to the brachial artery is rare but should be evaluated with a capillary refill of the fingernails. Normal is between 2-3 seconds and longer is concerning for a vasculature injury.
Imaging:
Imaging is an important part of the evaluation of elbow dislocations. X-rays are the first imaging ordered and an anteroposterior (AP) and lateral view should be obtained.
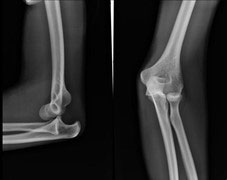
Posterior elbow dislocation lateral and AP view10
If there are no fractures on the X-ray, the elbow can be reduced immediately. If there are fractures, then the patient may require surgery and orthopedics should be consulted. Following reduction, the patient should have repeat X-rays to determine if the elbow was successfully reduced.

Normal alignment after the elbow has been reduced1
Treatment:
There are several methods for elbow reductions. Two common methods are the Parvin’s method and the Meyn & Quigley method12. The Parvin method involves the patient lying prone with the effected arm hanging off the table12. The physician places their hand behind their elbow and applies traction downward from wrist as seen below12. The Meyn & Quigley method is similar, but instead of placing one hand behind the patient’s elbow, they apply pressure to the olecranon while applying traction downward on the wrist as seen below12.
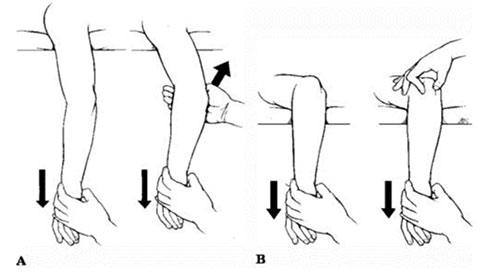
Parvin’s (A) and Meyn & Quigley (B) Reduction11
Management:
For a simple posterior elbow reduction, the patient is splinted at 90 degrees flexion for 1-2 weeks followed by physical therapy13. The patient should be seen in outpatient orthopedics 1 week after the injury and reduction for repeat X-rays13.
For complex elbow dislocations, surgery may require plates, pins, external fixation, and/or ligamentous repair13. The management depends on the severity of the injury and the operation performed13. Complex dislocations have an increased risk of neurovascular damage, reduced range of motion, instability, and pain13.
References:
- www.orthobullets.com/trauma/1018/elbow-dislocation
- www.ncbi.nlm.nih.gov/books/NBK559277/
- Dhillon MS, Gopinathan NR, Kumar V. Misconceptions about the three point bony relationship of the elbow. Indian J Orthop .2014; 48(5): p.453-7. doi:www.ncbi.nlm.nih.gov/pubmed/25298550
- vectormine.com/item/anatomy-of-elbow-skeletal-bone-structure-labeled-scheme-vector-illustration
- www.drmatanky.com/elbow-tendon-and-ligament-repair.html
- eorthopod.com/elbow-anatomy
- www.lecturio.com/concepts/elbow-joint
- sportsrehabcoach.com
- www.rch.org.au/fracture-education/evaluation/Evaluation
- radiopaedia.org/articles/elbow-dislocation?lang=us
- Egol K et al. Handbook of Fractures. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health, 2010.
- coreem.net/core/elbow-dislocation
orthoinfo.aaos.org/en/diseases--conditions/elbow-dislocation
For more information about our services or to schedule an appointment, call us at / / or click here to request an appointment online. We’ll respond to you as soon as possible.